
As deadlines loom, and doing becomes the necessary outcome of thinking, I want to reflect more on the science of SciArt: the connection between the disciplines, and the science of diabetes. (A quick disclaimer - from the outset this is the consideration of a lay-person, albeit one who is bound up in the experience as a student and a patient.)
The multiplicity of SciArt covers a vast space – from Stelarc implanting an ear on his arm (Stelarc, Stelarc.org. http://stelarc.org/?catID=20242 (1/2/17)), to Helen Storey’s Catalytic Clothing (Helen Story and Tony Ryan, Catalytic Clothing.org. http://www.catalytic-clothing.org (1/2/17)) - demonstrating how:
“Artwork and art process has the power to encapsulate some of the most complex debates of our times and, through offering a visceral experience, can traverse intellectual distances at light speed.” (pg. xv, Miah, A ed, 2008: Human Futures: Art in an Age of Uncertainty, Liverpool, Liverpool University Press)
Miah here highlights how the synthesis of the two disciplines has enabled a discourse of ideas to enter into a wider consciousness – fulfilling the social need for understanding, but also a deeper sense of engagement. Going further than simply seeing a practical use for a discovery, but interrogating the nature and the direction of that discovery. In a sense, we can see Art as a crucial part of the policing of Science. A view that Stephen Wilson elaborates – suggesting that artists are involved with “questioning the narratives of progress” (pg.11, Wilson, S. 2010: Art Science Now: How scientific research and technological innovation are becoming key to 21st century aesthetics. London. Thames & Hudson). This idea of questioning emphasises the nature of challenge in the relationship between the subjects, and points to a necessary tension in the relationship – a “critical dimension” (pg. 11 Ibid). Wilson goes further in suggesting that Science is seen as part of a ‘narrative’ – as a ‘world-view’ in itself that we – as a social-economic entity are complicit in if left unchecked. An approach Wilson cites in The Farm by Alexis Rockman (fig.1),

fig.1. Rockwell, A. 2000. The Farm. Alexis Rockman.net. http://alexisrockman.net/wonderful-world/ (1/2/17)
where we see the potential for environmental and genetic manipulation critiqued in relation to social and economic demands. This Wilson calls part of “a critique of the idealised version of science” (pg.12, Wilson. cited above)
Of course, this cannot work one-way, nor is it enough to suggest that Art is wholly critical of Science, Miah goes on:
“Artists have synthesized (sic) worlds into which the possibility of representation is infinite. They have found new forms of expression and have animated new architectures.” (pg. xv, Miah. cited above)
Reflecting on how the very forms of ‘Art’ have been challenged – pushing concepts of representation further – distorting the line between craft and technology, an act in which artists are complicit: “Artists also invent ways to visualise research results and make investigative process public” (pg.11 Wilson. cited above). It is this invention – this focus on form that pushes the artist into science, and makes science into art, this (dis)play of ideas formulated on a desire to explore, explain and discover meaning(s) that are hidden, or that resist our grasp. Art and Science do not exist in a vacuum, as Miah notes: “We cannot separate art from the cultural conditions of its production and, more widely, its role within the public sphere” (pg.xvi, Miah. cited above) – the same can be noted of Science – both arenas intersect within wider cultures, and if anything, the priority of SciArt is to ensure that intersection is not lost?
The intersection in my case is personal – infusing the medical science with my lived experience, finding a way to represent that experience, and engage meaningfully with a body of scientific discovery.
Diabetes itself is tricky (see here for a useful overview of the differences between types of Diabetes, and the site generally for loads of information Diabetes.co.uk, http://www.diabetes.co.uk/difference-between-type1-and-type2-diabetes.html (1/2/17)). I have type 1 diabetes - it’s an autoimmune disease, which means essentially my body is attacking itself.
“Ultimately auto-aggressive T cells invade pancreatic islets focusing destructive force on the beta cells that produce insulin” (pg.83, Wagner, D. The Role of T Cells in Type 1 Diabetes in Type 1 Diabetes - Pathogenesis, Genetics and Immunotherapy Downloaded from: http://www.intechopen.com/books/type-1-diabetespathogenesis-genetics-and-immunotherapy (30/12/16))
So - my T-cells (the body's police force if you like), are attacking my ß-cells, which reside in the Islets of Langerhans (which should be a Scottish Island - or at least a fantasy kingdom):
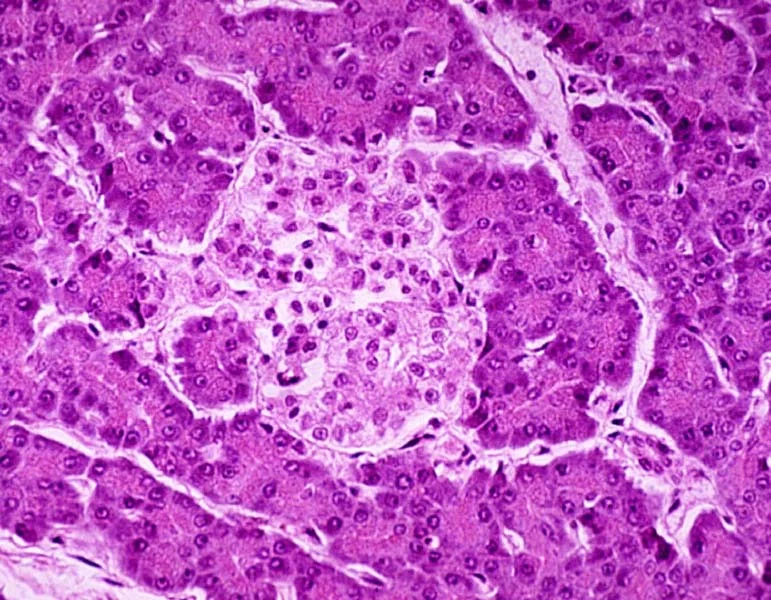
fig.2. Islets of Langerhans: Not a Scottish island (Bing images, wps.aw.com/wps/media/objects/443/454188/Fig19012.jpg (1/2/17))[Marieb, E: Essentials of Human Anatomy and Physiology. Pearson http://wps.aw.com/bc_marieb_ehap_10/178/45725/11705638.cw/index.html (1/2/17).]
Or, for a better understanding compare these Immunofluorescence stained images of healthy islets (fig 3) against a diabetic islet (fig 4)
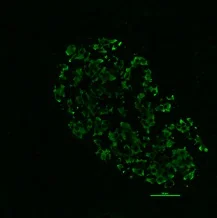
fig 3. Healthy pancreatic islet - showing insulin production.
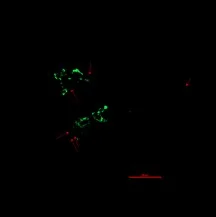
fig 4. Pancreatic islet with type 1 diabetes - showing insulin production. Provided by Dr Anneliese Flatt: clinical research centre Newcastle RVI.
· Cells counted manually for all different types
[Overview
· Immunofluorescence staining carried out in pancreas tissues for endocrine cell marker chromogranin A and pancreatic hormones viz. insulin, glucagon, somatstatin and pancreatic polypeptide A
· 15 type 1 diabetes tissues and 8 age-matched controls
· 50 islets per tissue imaged on the confocal microscope
· Islets defined as a cluster of more than 10 chromogranin-positive cells]
Looking at the damage – or the battleground it’s clear that the ß-cells are losing. This stops insulin production (or at least effective insulin production) - meaning I get a build-up of glucose in my blood if I don’t regulate it with external insulin… or exercise - maybe diet too? It also affects the ⍺-cells - the ones that produce glucagon when the bodies blood sugar drops too low.
But it turns out I do have some insulin left - my ß-cells are producing some, but its slow, and needs help - and it’s going to run out.
This means eventually I will be fully dependant on insulin. But studies have shown that the longer I can maintain ß-cell production of pro-insulin, and the better my glycaemic control, the better the health benefits.
“Therefore, all type 1 (and possibly many type 2) diabetic patients may benefit from any success in maintaining ß-cell (and thereby ⍺-cell) activity after onset of disease (21). From the data present here, the best current and practical method subsumes the best possible control for each diabetic patient. [pg.835]” (Steffes, M; Sibley; Jackson, M; Thomas, W: ß-Cell Function and the Develop of Diabetes-Related Complications in the Diabetes Control and Complications Trial. Diabetes Care, volume 26, number 3, March 2003)
The focus of the trial I am enrolled on with T1DUK is involved with exploring the potential impact on diabetes from an immunology approach. Basically, there is a two-pronged attack - with one drug (Liraglutide)used to aid the insulin secretion process and make the insulin I have more effective; alongside this is an infusion of an immune dampening drug to hold off the bodies attack on those ß-cells (effectively this gets the body’s immune system drunk, giving my ß-cells a break) This is assuming that I’m not taking one - or both placebos…
As well as the research I’m involved in, there are varied approaches to diabetes, including:
- Immunology
- Carbohydrate research
- The development & delivery of insulin
- Diet & impact
- Education (after-all each diabetic carries their own lab with them?)
So… where do I fit in?
- Patient - I am a diabetic type 1
- Research subject - immunology drug trials, but also daily testing and evaluation of my bodily responses
- Researcher & Diarist - daily blood tests and insulin dosages, personal blogs and journaling of experience, academic and visual research
- Diet - understanding and trial of daily carbohydrate intake, alternatives and options - including self medication using insulin and sugar
- Student - learning about the medical and practical impact of ‘new’ existence
- Illustrator - collection and development of research, and visual interpretation of experience
- Individual - personal experience
- Artist - collection, synthesis, interpretation and expression of information and experience
On a daily basis this means injections and regulation of my food, and an increased awareness of physical activity. This doesn’t mean I can/can’t eat certain foods (though sugar is something I keep away from - unless I’m low, when I don't - see already we’re getting confused here), but that I need to know what I’m eating and the effects. Generally, it’s all about the carbs - Carbohydrate breaks down into glucose - and that’s where the issues begin. Too much sugar build up can result in long term effects - such as blindness and amputation; too little results in comas (not commas - as a Lit graduate, that I could live with). But glucose provides energy, and can be used through exercise too; also, different carbs burn at different rates, and other foods can affect the way in which the body uses the carbs.
So now it’s about the planning, the maths, the chemistry, the biology, the medicine, the situation and the data. Regular tests let me know what’s going on inside me - and let me calculate what I need to inject - although I have to take into consideration what I’ve been doing, what I’m about to do, what time of day (‘cos the body isn’t necessarily consistent - ratios of insulin to carbohydrate change at the day, and the life, continue) on the basis of an analysis of the food I’m planning to eat. So, maths, apps, research, understanding and a bit of gut feeling all consolidate around each meal… and bedtime… and y’know, everything…
Surely there’s some art in there somewhere?